This is a challenging time but amid the concern, there are uplifting stories of how people are looking out for each other and communities pulling together. The children’s rainbows of hope in windows and the national clap for carers to celebrate the work of the NHS and care workers on Thursday were much appreciated.
Information is useful—but too much information can be unhelpful. I have limited news updates to new information from consensus sources. We don’t generally benefit from watching the news over and over. Try to focus instead on the things you need to get done. Value the rest of the time to relax with your family or friends and reach out to those who may not have such good support networks as you may have.
The bulletins below have some reassuring observations for our patients.
I hope that these help guide your practice while working differently.
1 )Statement “Gastrointestinal endoscopy in children and COVID 19 pandemic” – ESPGHAN Endoscopy Special Interest Group
“..elective procedures – especially those such as upper gastrointestinal (GI) endoscopy which is an ‘aerosol-generating procedure’ (AGP) – should be put on hold at present. Equally ileocolonoscopy, given that we know now that COVID-19 can be excreted in stools. Local and physician judgment should occur when determining which patients require urgent endoscopic diagnostic testing, but these should be kept to a minimum. Obviously, life-saving endoscopy such as GI bleeding and button battery ingestion are mandatory and should not be deferred. In the event of endoscopy being required a full personal exposure protection package should be worn by those in the immediate vicinity of the endoscopy including an FPP3 mask or equivalent”
Preliminary experience so far show that children under 12 years of age do not develop coronavirus pneumonia regardless of their immune status although they get infected and can spread the infection. Immune suppressed patients are not at risk for severe pulmonary disease compared with the general population.
2) Article “COVID-19 and paediatric inflammatory bowel diseases: global experience and provisional guidance (March 2020) from the Paediatric IBD Porto group of ESPGHAN”. see PDF attached https://bspghan.org.uk/jpgn-s-20-00391
Preliminary data for PIBD patients during COVID-19 outbreak are reassuring.
IBD per-se does not currently seem to be a risk factor for acquiring SARS-CoV-2, nor for a more severe infection. Standard IBD treatments including biologics should continue at present
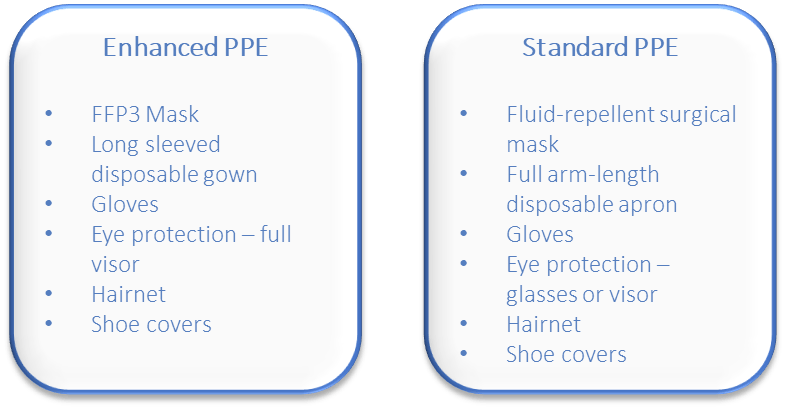
All upper GI endoscopy should be considered high risk and enhanced PPE is recommended for all patients, regardless of any risk stratification.
BSG also considers lower GI endoscopies to be aerosol generating procedures (AGP) but the evidence for this is less strong and there is insufficient evidence to consider these as high risk at the present time
Risk stratification of patients by symptoms and temperature is of limited value, given the widespread prevalence and incubation period of up to 14 days
We recognise the limited availability of PPE, especially FFP3 masks, and so case selection is critical, focussing only on emergency and absolutely essential procedures. Minimising the volume of emergency activity will help preserve PPE supply.
Notes on FFP3 masks and enhanced PPE
Proper fitting and testing prior to use
Although ‘single use’ can use for several hours if not removed/contaminated
FFP3 uncomfortable after prolonged wearing, may affect ease of procedure
Cannot e.g. use phone, visit, toilet, eat or drink once enhanced PPE is on
For COVID-positive patients – consider wearing full visor and surgical mask over FFP3 mask. This minimises risk of contamination of FFP3 mask and prolongs use
Further Key points for Optimal Practice
For known COVID-positive patients
Scope in designated, different area of the department
Designated, separate recovery area
Minimal furniture and equipment in room
Minimum essential staff in room
Remember
PPE is only part of the strategy to prevent and control transmission of infection
Team organisation –essential staff only in procedure room
Don’t share PCs, keyboards, phones etc – or clean thoroughly between users
The situation is rapidly evolving and this guidance may be updated regularly
Approaching a coughing patient, for example, even if COVID-19 has not been diagnosed. Protection including eye shield is needed.
Naso-gastric tube placement is an aerosol generating procedure (AGP). AGPSs are high risk. Full PPE is needed. Consider carrying out in a specified location.
Only emergency endoscopic procedures should be performed . No diagnostic work to be done and BSG guidance followed. Upper GI procedures are high risk AGPs and full PPE must be used
GI Endoscopy Activity and COVID-19: Next steps
INTRODUCTION
The BSG has produced recommendations(1,2) based on the best available evidence from China(3), Italy(4) and the USA(5) that show:
The virus causing COVID-19 is potentially present in all GI secretions.
That all endoscopic procedures, but particularly upper GI endoscopy, are aerosol generating procedures (AGP).
That transmission can occur at the time of endoscopy.
We have received reports that some centres are continuing to run booked endoscopy lists, requiring patients:
To travel.
To enter hospitals already treating significant numbers of COVID-19 patients.
To wait in areas that do not meet any of the Government’s social isolating directives.
For these reasons, the BSG has recommended that all but emergency procedures should stop immediately.
The main issues of contention remain whether Urgent 2 Week Wait (2WW) patients, (or Urgent Suspected Cancer (USC) patients in Scotland,) and patients already diagnosed as FIT positive under Bowel Cancer Screening Programs (BCSP), should be “paused” during the current crisis.
How any potential damage from delayed diagnosis can be mitigated.
2WW/USC, and BCSP referrals: Relative Diagnostic Yield. The Risks of Pausing
2WW/USC referrals – yield of cancer = 3%
Bowel cancer screening programmes (BCSP) (FIT+) – yield of cancer = 8-10%
Another, small percentage of patients will have advanced disease at the time of referral and the delay will not alter their prognosis, which unfortunately will already be very poor.
For this group, a delay of 3 months is unlikely to materially alter the risk of an adverse outcome.
Some of those who do not have established malignancy will have benign lesions such as polyps.
In the majority of these cases, progression to malignancy, if it occurs, may take years.
Conclusion: Very few patients are likely to come to harm from a pause of 3 months.
Risks of continuing 2WW/USC, BCSP and urgent referrals.
Removing polyps, particularly those over 1 cm, carries risks of haemorrhage and perforation often requiring admission to hospital.
During the COVID-19 crisis, ICU beds are unlikely to be available and even urgent surgical procedures will be restricted.
The risks of death from polypectomy usually quoted, are based on entry into a hospital operating under normal conditions, but not during a COVID-19 epidemic, where the risks of death will be significantly higher.
Patients who are diagnosed with cancer may not be offered surgery at the height of the epidemic. Their anxiety is likely to be equal to or even greater, than those with a positive FIT test whose colonoscopy is paused.
In addition:
All patients attending for a non-emergency endoscopy now enter a high-risk environment.
The benefit of endoscopy may be offset by the risk of COVID-19 infection to themselves.
The majority will be older than 60 years with higher mortality from COVID-19 if they become infected.
They become a potential risk to their families and contacts.
Patients with asymptomatic COVID-19 infection pose a significant risk to staff. By definition, their infection will not be detected before having a procedure.
The aerosol or droplets take up to an hour disperse, so they remain a risk to staff and other patients after they leave the room.
There is, therefore, little evidence that a pause of 3 months will pose a significant risk to the great majority of 2WW/USC or BCSP patients, although it is accepted that a small number of patients may have a delay in their diagnosis.
On the other hand, a much larger number of patients and staff will be put at significant risk of COVID-19 if the 2WW/USC and BCSP is continued even at a scaled-down level.
Conclusions and Actions.
Stop all non-emergency endoscopy immediately.
Triage plan to identify patients who fall into the emergency category. The evidence base for this is laid out in previous BSG documents. (1) and follows experience from China(3), Italy(4) and the USA(5).
List all patients on to a separate Urgent Deferred Waiting List to prioritise their investigation when services resume.
To: Free-up the maximum possible inpatient and critical care capacity.
Prepare for, and respond to, the anticipated large numbers of COVID-19 patients who will need respiratory support.
Support staff, and maximise their availability. Play our part in the wider population measures newly announced by Government.
Stress-test operational readiness.
Remove routine burdens, so as to facilitate the above
2. Letter from CMO Stephen Powis (attached)
Advice concerning those who are or may be at increased risk of severe illness from COVID-19
Please see a letter suitable to be sent to families in annex 3.
Patients on immunosuppression therapies sufficient to significantly increase risk of infection have been outlined in the BSG Guidance which has been updated today 23/3/20.
Our advice today when we called families of children and young people with IBD in the high risk category, (see guidance – while on steroids prednisolone equivalent to or greater than 20mg, or within 6 weeks of starting a biological therapy, or with severe active disease), was to reassure that Covid19 appears not to cause such severe disease in children and young people.
We reinforced that patients should continue their usual treatment, including infusion therapy, and to continue to contact their IBD team by phone if they have symptoms eg fever, typical features of a relapse. The team will assess each patient case by case and advise accordingly.
3. HOMECARE (Home Parenteral nutrition) advice from 23/3/20 issued by Susan Gibert, who is leading on COVID-19 for Homecare
This has been sent to all regional homecare leads who will disseminate to the trusts.
NHSE contract – CCGs (12 week rule)
In TVW I have gained agreement that NHSE and CCGs will not be expecting the homecare activity to have been recorded within the usual time frames. It might be a good idea to do the same in your regions.
Delivery windows – relaxation of expectation I have agreed with NCHA members that the NHS will not be expecting homecare providers to ‘hit’ their 2 hour delivery windows. Deliveries may need to move to all day windows in the near future, and if this is necessary can we agree to be supportive please? Homecare providers and hospitals are asked to be extra vigilant with the delivery address details as patients may no longer be at their usual work or residential addresses.
Emergency deliveries
We may reach a time where same day, next day and emergency deliveries are no longer possible. We may need to consider adjusting buffer stock in patients’ homes. At the moment, we do not have the reassurance that there is stock to do this, but it is something that we need to bear in mind for the coming weeks.
Phone Lines Homecare providers are experiencing high volumes of calls, this has led to longer wait times. Patients are also reporting that their hospital clinical teams are no longer manning some NHS helplines (as specialist nurses are being called to ward and other duties). Please can you ensure that you use the correct line of communication as per local agreements. If the route of contact is via your BDM, RBM etc, please can you refrain from ringing the homecare providers?
Equally if your CNS staff are being called to the front line, please can you ensure that the homecare providers have a contact number or email for an alternative contact? If in doubt, the pharmacy homecare team will be contacted for all enquiries that have not been dealt with in a timely manner. In TVW we will be ensuring that the pharmacy contacts are up to date, if you could do the same, that would be great.
Dr Sue Protheroe, Consultant Paediatric Gastroenterologist, Birmingham Women’s and Children’s Hospital. Birmingham. B4 6NH. U.K. Tel 0044 121 333 8705 Fax 0044 121 333 8701 Chair NHS England Clinical Reference Group, Paediatric Medicine. President of British Society of Paediatric Gastroenterology, Hepatology & Nutrition.